The sternoclavicular (SC) joint, a delicate articulation where the clavicle meets the sternum, demands a meticulous approach to imaging. Accurate X-ray positioning is the linchpin for obtaining detailed and diagnostically valuable images of this vital joint. In this blog, we delve into the intricacies of SC joint X-ray positioning, unveiling the art of precision imaging.
Table of Contents
Anatomy of the Sternoclavicular Joint and Its Role in Shoulder Function
The sternoclavicular joint (SCJ) is a critical but often overlooked component of the shoulder complex, playing a vital role in upper limb mobility and stability. Understanding the anatomy of the SCJ and its role in shoulder function provides insight into how this small yet significant joint supports the wide range of motion required for daily activities.
Anatomy of the Sternoclavicular Joint
1. Joint Structure
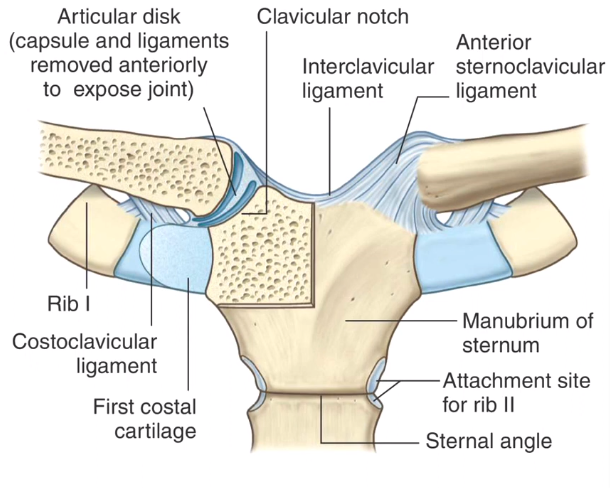
The sternoclavicular joint is a saddle-type synovial joint that connects the upper limb to the axial skeleton. It is located where the clavicle (collarbone) meets the manubrium of the sternum (breastbone) and the first costal cartilage.
- Articulating Surfaces: The joint involves the sternal end of the clavicle, the manubrium of the sternum, and the first rib’s cartilage. The surfaces are covered with fibrocartilage, unlike the hyaline cartilage found in most other synovial joints, providing greater durability and resistance to wear.
- Joint Capsule: A fibrous capsule surrounds the joint, lined with a synovial membrane that secretes synovial fluid to lubricate the joint and facilitate smooth movement.
2. Ligaments of the Sternoclavicular Joint
Several ligaments reinforce the SCJ, contributing to its stability:
- Anterior and Posterior Sternoclavicular Ligaments: These ligaments provide anterior and posterior stability, preventing excessive forward and backward displacement of the clavicle.
- Interclavicular Ligament: Spanning between the two clavicles above the sternum, this ligament restricts excessive downward movement of the clavicle.
- Costoclavicular Ligament: Located between the clavicle and the first rib, this strong ligament is crucial for stabilizing the joint by limiting elevation and controlling overall clavicular movement.
3. Articular Disc
An articular disc of fibrocartilage divides the SCJ into two separate compartments, enhancing joint stability and shock absorption. The disc acts as a pivot point for movement and helps distribute forces transmitted through the clavicle.
Role of the Sternoclavicular Joint in Shoulder Function
The SCJ is pivotal in enabling the wide range of motion required for shoulder and arm movements. It is the only direct articulation between the upper limb and the trunk, providing a critical link that facilitates various shoulder and arm activities.
1. Movement and Range of Motion
The SCJ allows for multiple movements that contribute to shoulder mobility:
- Elevation and Depression: This movement occurs when raising or lowering the shoulders, such as during shrugging. The SCJ allows the clavicle to move upward (elevation) by about 30-40 degrees and downward (depression) by about 10 degrees.
- Protraction and Retraction: The SCJ allows the clavicle to move forward (protraction) and backward (retraction). This is essential for actions like reaching forward or pulling the shoulders back.
- Rotation: The clavicle can rotate around its axis approximately 30-50 degrees, especially during activities like arm elevation, allowing smooth upward movement of the shoulder.
2. Force Transmission and Load Distribution
The SCJ plays a vital role in transmitting forces from the upper limb to the axial skeleton. For example, when pushing, pulling, or lifting objects, forces are transmitted through the SCJ, distributing stress and minimizing potential damage to the shoulder girdle.
3. Stability and Dynamic Support
The SCJ, despite its relatively small size, provides significant stability to the shoulder girdle. Its ligaments and articular disc help stabilize the clavicle during various dynamic movements, ensuring that the shoulder remains securely attached to the body during strenuous activities like throwing or lifting.
4. Coordination of Shoulder Movements
The SCJ works in concert with other shoulder joints, including the acromioclavicular (AC) joint, glenohumeral joint, and scapulothoracic articulation, to coordinate complex shoulder movements. Proper function of the SCJ is essential for maintaining smooth and coordinated shoulder motion, which is crucial for athletic activities and daily tasks.
Clinical Relevance of the Sternoclavicular Joint
Due to its role in shoulder function, dysfunction or injury to the SCJ can significantly impact overall shoulder mechanics. Conditions such as arthritis, dislocation, and ligament sprains can affect the SCJ, leading to pain, reduced mobility, and impaired shoulder function.
- Dislocations: Although rare, SCJ dislocations can occur, particularly from traumatic injuries. Anterior dislocations are more common and usually result from direct trauma to the shoulder.
- Arthritis: Degenerative changes in the SCJ can lead to osteoarthritis, causing pain and limiting movement, particularly during shoulder elevation.
- Infections and Inflammations: The SCJ can be affected by infections, such as septic arthritis, which can cause severe pain and swelling, often requiring medical intervention.
The sternoclavicular joint, though small, is fundamental to shoulder function and overall upper limb mobility. Its unique anatomy allows for a By understanding the SCJ’s structure, mechanics, and clinical significance, healthcare professionals can better diagnose and manage conditions affecting shoulder function. Proper care and attention to this joint are crucial for maintaining optimal upper body movement and function.
Indications for Sternoclavicular Joint (SC Joint) X-rays and Specific Information Obtained
SC joint X-rays are an essential diagnostic tool used to evaluate various conditions affecting the sternoclavicular joint, a critical part of the shoulder complex. These X-rays help healthcare professionals assess the joint’s anatomy, detect abnormalities, and plan appropriate treatment strategies. Here’s an in-depth look at the indications for SC joint X-rays and the specific information they can provide.
Indications for SC Joint X-rays
SC joint X-rays are primarily indicated when patients present with symptoms that suggest problems in the sternoclavicular joint. Common indications include:
1. Trauma and Injury Assessment
- Indication: X-rays are commonly ordered when there is a history of trauma, such as a direct blow to the chest, a fall onto an outstretched arm, or vehicular accidents, which can lead to SC joint dislocation, subluxation, or fractures.
- Information Obtained: X-rays help visualize the extent of joint dislocation (anterior or posterior) and any associated fractures of the clavicle or manubrium. They provide critical information about the alignment of the joint and the severity of the injury.
2. Joint Pain and Swelling
- Indication: Chronic or acute pain localized to the SC joint, often accompanied by swelling, tenderness, or limited range of motion, can indicate inflammatory or degenerative conditions.
- Information Obtained: X-rays can reveal joint space narrowing, subchondral sclerosis, and the presence of osteophytes, which are indicative of osteoarthritis or other inflammatory conditions like rheumatoid arthritis.
3. Suspected Infections
- Indication: SC joint infections, such as septic arthritis, present with symptoms like severe pain, redness, warmth, and fever. These infections are more common in individuals with a history of intravenous drug use, diabetes, or immunosuppression.
- Information Obtained: X-rays can show joint space widening, bone erosion, and soft tissue swelling, which are suggestive of infection. However, more advanced imaging techniques (e.g., MRI, CT) may be required for a detailed assessment.
4. Joint Deformity or Mass
- Indication: Deformities or palpable masses around the SC joint, such as those caused by tumors, cysts, or hypertrophic changes, necessitate further investigation.
- Information Obtained: X-rays can help identify abnormal growths, calcifications, or bony expansions that may suggest benign or malignant processes, such as osteochondromas or bone metastases.
5. Degenerative Joint Disease
- Indication: Patients with degenerative joint disease may experience chronic pain, stiffness, and reduced joint mobility, particularly in older adults.
- Information Obtained: X-rays can reveal changes typical of osteoarthritis, including joint space narrowing, osteophyte formation, and subchondral cysts, aiding in confirming the diagnosis.
6. Assessment of Congenital Abnormalities
- Indication: Congenital conditions, such as Sprengel’s deformity or cleidocranial dysplasia, may involve abnormalities in the SC joint that require evaluation.
- Information Obtained: X-rays can highlight congenital malformations of the clavicle or sternum, aiding in understanding the joint’s involvement in the broader anatomical abnormality.
Specific Information Obtained from SC Joint X-rays
SC joint X-rays provide valuable insights into the joint’s anatomy and any pathological changes, helping guide diagnosis and treatment. Here are the specific details that can be derived:
- Joint Alignment and Positioning: X-rays can clearly show the alignment of the SC joint, identifying dislocations (anterior or posterior) and subluxations. Anterior dislocations are more visible on standard views, while posterior dislocations may require additional imaging techniques for clearer visualization.
- Bony Structures and Fractures: X-rays provide detailed images of the bony components of the SC joint, including the clavicle, manubrium, and first rib. They can detect fractures, bone spurs, and other structural abnormalities that may be causing symptoms.
- Joint Space Evaluation: The joint space width can be assessed to identify conditions like joint narrowing associated with arthritis or joint widening indicative of dislocation or infection. Changes in the joint space are critical markers for diagnosing degenerative or inflammatory conditions.
- Presence of Calcifications or Foreign Bodies: Calcifications around the SC joint, often seen in conditions like Tietze syndrome or trauma, can be detected on X-rays. These calcifications may contribute to pain and restricted movement.
- Erosions and Sclerosis: Erosions along the joint surfaces suggest inflammatory processes such as septic arthritis or rheumatoid arthritis, while subchondral sclerosis indicates chronic joint stress or osteoarthritis.
- Soft Tissue Abnormalities: While soft tissue visualization is limited on standard X-rays, significant abnormalities like swelling or masses can sometimes be inferred from distortions around the joint area.
- Evaluation of Post-Surgical Changes: X-rays are also used post-surgery to assess the position of any hardware, check for proper joint alignment, and monitor for complications such as hardware loosening or migration.
SC joint X-rays are a valuable diagnostic tool, providing critical information about the joint’s structure, alignment, and any pathological changes. They are essential for diagnosing various conditions, from trauma and arthritis to infections and congenital abnormalities, helping healthcare providers develop effective treatment plans. Proper interpretation of these images is crucial for accurate diagnosis and optimal patient care, emphasizing the importance of understanding SC joint anatomy and its role in shoulder function.
Alternative Imaging Techniques for Evaluating the Sternoclavicular (SC) Joint: Advantages and Disadvantages
While X-rays are often the first-line imaging modality for evaluating the SC joint, several other imaging techniques can provide more detailed insights, especially in complex cases. Alternative imaging techniques, including CT scans, MRI, ultrasound, and nuclear medicine, each have unique strengths and limitations. Here’s an in-depth look at these methods and a comparison of their advantages and disadvantages.
1. Computed Tomography (CT) Scan
Advantages:
- High-Resolution Images: CT scans provide detailed cross-sectional images of the SC joint, offering excellent visualization of bone structures, fractures, and joint dislocations.
- 3D Reconstruction: CT allows for 3D reconstructions, which are valuable in complex cases involving dislocations or fractures, aiding in surgical planning and assessment of injury severity.
- Superior to X-rays for Bone Detail: CT is particularly effective in identifying subtle fractures, erosion, and bony abnormalities that may not be visible on standard X-rays.
Disadvantages:
- Higher Radiation Exposure: Compared to standard X-rays, CT scans involve a significantly higher dose of radiation, which is a concern, especially in younger patients or those requiring multiple scans.
- Limited Soft Tissue Contrast: Although excellent for bone evaluation, CT scans have limited capability in distinguishing soft tissue abnormalities such as ligament or cartilage injuries.
- Cost and Accessibility: CT scans are more expensive and less accessible than X-rays, particularly in resource-limited settings.
2. Magnetic Resonance Imaging (MRI)
Advantages:
- Excellent Soft Tissue Contrast: MRI provides superior soft tissue imaging, making it ideal for evaluating ligaments, cartilage, muscles, and detecting inflammation, infections, or tumors in the SC joint.
- No Radiation: MRI does not use ionizing radiation, making it a safer option for repeated imaging, especially in young patients or those with radiation sensitivities.
- Detailed Assessment of Inflammatory Conditions: MRI is highly sensitive in detecting conditions like septic arthritis, osteomyelitis, or rheumatoid arthritis, showing bone marrow edema, joint effusion, and soft tissue involvement.
Disadvantages:
- Longer Examination Time: MRI scans are time-consuming, often taking 30 minutes to an hour, which can be challenging for patients with pain, claustrophobia, or limited ability to remain still.
- Higher Cost: MRI is more expensive than other imaging techniques, which may limit its availability and routine use in initial SC joint evaluations.
- Contraindications: Patients with certain implants, pacemakers, or metallic foreign bodies cannot undergo MRI due to the strong magnetic fields.
3. Ultrasound
Advantages:
- Dynamic Assessment: Ultrasound allows for real-time evaluation of the SC joint during movement, which can be helpful in assessing joint instability or guiding injections.
- Soft Tissue Visualization: It provides good visualization of soft tissue structures, including ligaments, tendons, and synovial fluid, making it useful in detecting effusions or synovitis.
- No Radiation and Cost-Effective: Ultrasound is a safe, cost-effective, and widely accessible imaging modality without the risks associated with radiation exposure.
Disadvantages:
- Operator Dependent: The quality of ultrasound imaging is highly dependent on the skill and experience of the operator, which can affect diagnostic accuracy.
- Limited Bone Detail: Ultrasound is not effective for detailed bone evaluation; it cannot visualize fractures or bony abnormalities as clearly as CT or MRI.
- Limited Field of View: Ultrasound provides a limited and superficial field of view, which may not capture deep-seated abnormalities within the SC joint.
4. Nuclear Medicine Scans (Bone Scintigraphy)
Advantages:
- Sensitive to Bone Metabolic Changes: Bone scans can detect increased bone activity associated with infection, inflammation, or tumors before structural changes are visible on X-rays or CT scans.
- Useful in Chronic Conditions: It is particularly helpful in diagnosing chronic inflammatory conditions like rheumatoid arthritis or osteomyelitis, providing a whole-body overview of joint involvement.
Disadvantages:
- Limited Specificity: While highly sensitive, bone scans lack specificity and may not clearly distinguish between different pathological processes, such as infection versus inflammation.
- Radiation Exposure: Bone scintigraphy involves exposure to radiation, although generally lower than CT but higher than plain X-rays, making it less ideal for repeated imaging.
- Time-Consuming and Expensive: The procedure requires the injection of radioactive tracers and several hours of imaging, making it less convenient and more costly than other modalities.
Comparison of Alternative Imaging Techniques
| Imaging Modality | Main Advantages | Main Disadvantages | Best Used For |
|---|---|---|---|
| CT Scan | Detailed bone imaging, 3D reconstructions | High radiation, poor soft tissue contrast | Complex fractures, dislocations, surgical planning |
| MRI | Excellent soft tissue detail, no radiation | High cost, longer scan time | Ligament injuries, infections, inflammation |
| Ultrasound | Real-time imaging, no radiation | Operator dependent, limited bone detail | Joint effusion, guided injections |
| Bone Scintigraphy | Sensitive to bone metabolic changes | Non-specific, radiation exposure | Chronic inflammation, infection detection |
The choice of imaging depends on the specific clinical scenario, the patient’s condition, and the need for detailed anatomical versus functional information, emphasizing the importance of selecting the appropriate modality to ensure accurate diagnosis and effective management of SC joint pathologies.
Navigating the Anatomy: Techniques for Accurate SC Joint X-ray Positioning
The sternoclavicular (SC) joint, a crucial articulation where the clavicle meets the sternum, plays a pivotal role in shoulder and upper limb function. Accurate imaging of the SC joint is essential for diagnosing various conditions, including dislocations, fractures, or degenerative changes. Navigating the anatomy through precise X-ray positioning is the key to obtaining informative images. Let’s delve into the techniques that radiographers employ for accurate SC joint X-ray positioning.
1. Understanding SC Joint Anatomy: Foundation for Precision
- Importance of Anatomy: Radiographers must have a comprehensive understanding of the SC joint’s anatomy, including the sternal and clavicular facets.
- Visualizing Joint Spaces: Recognizing normal joint spaces and bony landmarks forms the foundation for accurate positioning.
2. Patient Positioning for AP SC Joint View
- Patient Alignment: Position the patient in an upright stance with their back against the X-ray detector.
- Mid-Sagittal Plane Alignment: Ensure that the patient’s mid-sagittal plane aligns with the center of the X-ray beam.
3. Central Ray Placement: Targeting the SC Joint
- Central Ray Alignment: Direct the central ray perpendicular to the mid-sagittal plane and centered on the SC joint.
- Optimal Collimation: Employ collimation to focus the X-ray beam precisely on the joint area, minimizing unnecessary radiation exposure.
4. Evaluating Bilateral SC Joints: Comparative Analysis
- Bilateral Assessment: Capture both SC joints in a single image for comparative analysis.
- Symmetry Checks: Confirm symmetrical positioning of the clavicles and joint spaces, aiding in the detection of abnormalities.
5. Oblique SC Joint Views: Specialized Assessment
- Oblique Positioning: Rotate the patient 10-15 degrees obliquely for specialized SC joint assessment.
- Facilitating Joint Space Visualization: Oblique views help visualize joint spaces and facets not as clearly visible in the AP view.
6. Visualizing Medial Clavicular Borders: SC Oblique Technique
- Medial Clavicle Visualization: Angle the X-ray tube to visualize the medial borders of the clavicles.
- Assessing Joint Alignment: Evaluate joint alignment and potential abnormalities with enhanced clarity.
7. Patient Education and Communication: Minimizing Movement
- Clear Instructions: Educate the patient on the importance of remaining still during the procedure.
- Minimizing Artifacts: Minimize motion artifacts by ensuring patient cooperation and understanding.
8. Supine Positioning for Trauma Cases: Alternative Approach
- Supine Stance: In cases of trauma or patient discomfort, a supine position may be employed.
- Minimizing Discomfort: This alternative position minimizes patient discomfort while providing diagnostic images.
9. Continuous Training for Radiographers: Skill Refinement
- Training Programs: Radiographers should undergo continuous training on SC joint positioning techniques.
- Adapting to Diverse Cases: Training ensures adaptability to variations in patient anatomy and specific cases.
10. Quality Control and Image Review: Ensuring Accuracy
- Post-Processing Review: Implement post-processing techniques to enhance image quality.
- Regular Quality Control: Conduct regular quality control assessments to ensure consistent and accurate SC joint imaging.
By navigating the anatomy with these techniques, healthcare professionals can consistently obtain diagnostic images that contribute to the effective evaluation and management of SC joint conditions.
Also read: Lordotic Chest X-ray
Advanced Strategies in SC Joint X-ray Positioning for Radiographers
The sternoclavicular (SC) joint, a nexus of intricate anatomy and potential pathology, demands advanced strategies in imaging for thorough assessments. Radiographers, as key players in this process, can elevate their practice by incorporating advanced techniques into SC joint X-ray positioning. Let’s explore these strategies to enhance precision and diagnostic capabilities.

1. Dynamic Stress Views: Unveiling Instabilities
Traditional static views may not fully capture dynamic joint behavior. Incorporating stress views, where the patient actively moves their shoulders, can unveil subtle instabilities or abnormalities in the SC joint. This dynamic perspective provides a more comprehensive assessment, especially beneficial in cases of suspected ligamentous injuries or joint laxity.
2. Bilateral Stress Views: Symmetry Analysis
When exploring dynamic stress views, considering bilateral stress imaging provides a holistic understanding of joint symmetry. Comparing the behavior of both SC joints during stress maneuvers aids in identifying disparities, guiding clinicians in determining the nature and severity of abnormalities.
3. Advanced Collimation Techniques: Precision in Focus
Fine-tuning collimation is more than a routine practice; it’s an advanced strategy for optimizing image quality and reducing unnecessary radiation exposure. Implementing edge-enhancing collimation techniques directs the X-ray beam precisely to the SC joint area, minimizing scatter and enhancing the clarity of crucial anatomical details.
4. CT Arthrography Correlation: Fusion of Modalities
In certain diagnostic scenarios, correlating SC joint X-rays with computed tomography (CT) arthrography can provide a more comprehensive evaluation. This fusion of modalities offers detailed anatomical insights, particularly in complex cases where traditional X-rays alone may not suffice.
5. SC Joint Ultrasound Guidance: Real-Time Visualization
Integrating ultrasound guidance during SC joint imaging provides real-time visualization of soft tissues and potential pathologies. Radiographers can collaborate with sonographers to align the ultrasound probe precisely, enhancing the accuracy of the procedure and allowing for simultaneous assessment of dynamic joint movements.
6. Cone Beam CT: Three-Dimensional Insights
For an even more detailed assessment, especially in cases demanding a three-dimensional perspective, cone beam CT can be considered. This advanced imaging modality provides volumetric data, offering comprehensive insights into the SC joint’s complex anatomy and aiding in precise diagnosis.
7. Radiographic Tomosynthesis: Layered Imaging
Radiographic tomosynthesis, akin to CT scanning but with reduced radiation exposure, allows for layered imaging of the SC joint. This advanced technique provides multiple sectional views, enabling radiographers to navigate through anatomical layers and detect abnormalities that may be obscured in traditional X-rays.
8. Digital Tomosynthesis: Enhancing Detail Recognition
Digital tomosynthesis takes the layered approach a step further, offering enhanced depth resolution and improved detail recognition. Radiographers can utilize this advanced technology to unravel subtle anomalies within the SC joint, contributing to more accurate diagnoses.
9. Weight-Bearing Views: Mimicking Real-Life Conditions
Simulating real-life conditions by incorporating weight-bearing views during SC joint imaging can reveal discrepancies that may be concealed in standard positions. This strategy is particularly relevant in cases where joint abnormalities manifest or worsen under the influence of gravitational forces.
10. Artifact Reduction Protocols: Elevating Image Quality
Implementing advanced artifact reduction protocols is crucial for elevating image quality. Radiographers can explore techniques such as metal artifact reduction algorithms to minimize interference from implants or other metallic structures, ensuring clearer visualization of the SC joint.
By embracing dynamic approaches, fusion of modalities, and cutting-edge technologies, they contribute to a more comprehensive and nuanced understanding of the SC joint, empowering healthcare teams to deliver precise diagnoses and tailored treatment plans.
A Radiologist’s Perspective on SC Joint X-ray Positioning Challenges

Navigating the complexities of SC joint X-ray positioning presents unique challenges, and from a radiologist’s standpoint, addressing these challenges is crucial for accurate diagnoses and effective patient care. Let’s delve into the perspective of a radiologist on the specific positioning challenges encountered when imaging the sternoclavicular (SC) joint.
1. Superimposition of Anatomical Structures:
- Challenge: The SC joint is anatomically intricate, nestled amidst vital structures, leading to potential superimposition.
- Radiologist’s Insight: Superimposition can obscure subtle abnormalities, making it imperative for radiographers to employ precise positioning techniques that minimize overlap and enhance clarity.
2. Alignment Variability in Trauma Cases:
- Challenge: Trauma cases often involve variations in patient positioning due to pain or injury, complicating the alignment of the SC joint.
- Radiologist’s Insight: Consistent alignment is crucial for accurate assessments. Radiographers should adapt techniques to accommodate trauma patients, ensuring diagnostic quality without exacerbating discomfort.
3. Suboptimal Visualization of Ligaments:
- Challenge: Ligaments around the SC joint, vital for stability, may not be adequately visualized in standard views.
- Radiologist’s Insight: Advanced positioning techniques, dynamic views, or even correlation with other imaging modalities like MRI can provide a more comprehensive evaluation of ligamentous structures.
4. Overcoming Patient Discomfort:
- Challenge: Achieving optimal positioning may be hindered by patient discomfort, especially in cases where dynamic views or stress imaging is necessary.
- Radiologist’s Insight: Radiographers play a key role in patient communication, ensuring that patients understand the importance of positioning while maintaining their comfort. This collaboration is essential for successful imaging.
5. Distinguishing Between Normal Variants and Pathology:
- Challenge: Normal anatomical variations in the SC joint can sometimes mimic pathology.
- Radiologist’s Insight: Radiographers should be attuned to the subtle differences and employ precise positioning to aid radiologists in distinguishing between normal variants and potential pathology.
6. Limited Visualization in Pediatric Cases:
- Challenge: Pediatric cases pose unique challenges due to smaller anatomy and potential difficulties in achieving optimal positioning.
- Radiologist’s Insight: Tailored approaches for pediatric patients, such as modifications in equipment or positioning, are essential to ensure clear visualization and accurate assessments.
7. Complexity in Diagnosing Instabilities:
- Challenge: Detecting subtle instabilities, crucial for accurate diagnoses, can be complex in static views.
- Radiologist’s Insight: Radiographers should explore dynamic stress views or weight-bearing positions, providing radiologists with valuable information on joint stability under different conditions.
8. Balancing Image Quality and Radiation Exposure:
- Challenge: Achieving optimal image quality while minimizing radiation exposure is a perpetual balancing act.
- Radiologist’s Insight: Radiographers should adhere to stringent collimation practices, employ modern technologies that reduce artifacts, and advocate for low-dose techniques to ensure patient safety without compromising diagnostic clarity.
9. Complexities in Obese Patients:
- Challenge: Obesity can introduce complexities in achieving optimal positioning and image quality.
- Radiologist’s Insight: Radiographers should collaborate with patients, employing creative solutions and adapting positioning techniques to accommodate the challenges posed by obesity.
10. Artifact Management in Metal Implants:
- Challenge: Metal implants, common in the clavicular region, can introduce artifacts that affect image interpretation.
- Radiologist’s Insight: Radiographers should be well-versed in artifact reduction protocols, utilizing techniques that minimize interference from metallic structures and ensuring accurate diagnostic interpretation.
A radiologist’s perspective underscores the importance of addressing specific challenges in SC joint X-ray positioning. Collaborative efforts between radiographers and radiologists are essential for overcoming these challenges and achieving optimal imaging outcomes that contribute to precise diagnoses and effective patient management.
Practical Tips for Improving SC Joint X-ray Positioning Techniques
Proper positioning techniques are crucial when performing Sternoclavicular (SC) joint X-rays to ensure clear, diagnostic-quality images. Accurate positioning minimizes the need for repeat exposures, reducing radiation dose and discomfort for the patient while enhancing the visibility of the SC joint structures. Here are practical tips to improve SC joint X-ray positioning techniques:
1. Understand the Anatomy and Indications
- Familiarize with SC Joint Anatomy: Understanding the SC joint’s anatomy is key to positioning correctly. The SC joint connects the sternum (breastbone) to the clavicle (collarbone), and its alignment can vary based on patient anatomy and positioning.
- Recognize Indications for Imaging: Common indications include trauma, dislocation, arthritis, infection, or pain localized to the SC joint. Tailoring positioning to the specific clinical indication can improve the diagnostic yield of the X-ray.
2. Use Correct Positioning Techniques
- Standard Views: The most common views for SC joint X-rays are the Anteroposterior (AP) view, Oblique views (right and left), and Serendipity view. Each has unique positioning requirements:
- AP View: Position the patient upright or supine with the shoulders relaxed. Center the X-ray beam at the level of the SC joint with the central ray perpendicular to the cassette. This view provides a bilateral assessment of the joints.
- Oblique Views (Right and Left): Position the patient at a 15-20 degree angle, turning the unaffected side closer to the cassette. This technique allows for a clearer view of the joint being evaluated and reduces superimposition of structures.
- Serendipity View: This view is specifically designed for SC joint evaluation. The patient lies supine with the X-ray beam angled 40 degrees cephalad. It provides a clear visualization of both SC joints, aiding in the assessment of dislocations.
3. Optimize Patient Comfort and Stability
- Ensure Patient Comfort: A comfortable patient is more likely to remain still, reducing motion artifacts. Provide pillows or positioning aids to support the head, neck, and shoulders.
- Stabilize the Patient: Use sandbags, positioning wedges, or straps to secure the patient in the desired position. Stability is especially important for patients with pain or difficulty maintaining positioning.
4. Adjust Beam Alignment and Angulation
- Accurate Beam Centering: Center the X-ray beam directly over the SC joint or slightly medial to the joint being examined. Incorrect centering can lead to poorly visualized joints or missed pathology.
- Correct Angulation: Adjust the X-ray tube angulation based on the chosen view to minimize superimposition of surrounding structures. For example, in the Serendipity view, a cephalad angulation of 40 degrees enhances joint visibility.
5. Use Proper Collimation and Exposure Settings
- Collimate Appropriately: Narrow the X-ray beam to focus on the SC joint area, which reduces patient radiation exposure and improves image contrast.
- Optimize Exposure Parameters: Use the correct kVp (kilovoltage peak) and mAs (milliampere-seconds) settings based on patient size and body habitus. Higher kVp can reduce contrast but is useful for penetrating dense areas.
6. Employ Lead Shielding and Radiation Safety Measures
- Use Lead Aprons: Provide lead aprons or thyroid shields to protect the patient from unnecessary radiation exposure, especially in pediatric or repeat imaging scenarios.
- Minimize Repeat Exposures: Proper positioning and exposure settings reduce the need for repeat X-rays, enhancing patient safety.
7. Communicate with the Patient
- Provide Clear Instructions: Explain the procedure and positioning to the patient in simple terms, instructing them to hold their breath during exposure to reduce motion blur.
- Reassure and Guide: Reassure anxious patients and provide guidance throughout positioning to keep them at ease, which helps achieve optimal imaging results.
8. Use Positioning Aids and Markers
- Markers: Place right (R) or left (L) markers on the images to indicate the side being examined, which aids in proper interpretation and documentation.
- Positioning Devices: Use wedges, sponges, or foam pads to maintain the correct angulation and support the patient comfortably.
9. Review Images Immediately
- Preliminary Image Check: After obtaining the X-ray, review the image for positioning accuracy and diagnostic quality before dismissing the patient. This helps identify positioning errors early, allowing for immediate correction without requiring the patient to return.
- Adjust Positioning as Needed: If the SC joint is not well-visualized, adjust the positioning and retake the image promptly to minimize patient time and discomfort.
Proper positioning is fundamental to obtaining high-quality SC joint X-rays that provide valuable diagnostic information. By understanding the anatomy, using correct techniques, and ensuring patient comfort and safety, radiologic technologists can significantly improve imaging outcomes. Employing these practical tips will enhance the clarity, accuracy, and effectiveness of SC joint X-rays in clinical practice.
Common Errors in SC Joint X-ray Positioning and Their Consequences
Proper positioning in SC (Sternoclavicular) joint X-rays is essential to obtain clear and diagnostically accurate images. Errors in positioning can compromise image quality, reduce diagnostic accuracy, and potentially lead to misdiagnosis or the need for repeat imaging, increasing patient radiation exposure. Here are some common errors in SC joint X-ray positioning and their consequences:
1. Incorrect Centering of the X-ray Beam
- Error: The X-ray beam is not centered precisely on the SC joint or is misaligned laterally or vertically.
- Consequences: Miscentering can result in part of the SC joint being cut off from the image or obscured by surrounding structures, making it difficult to assess the joint fully. This can lead to missed diagnoses of dislocations, fractures, or degenerative changes.
2. Improper Patient Angulation
- Error: The patient is not angled correctly for oblique views, or the body is rotated excessively or insufficiently.
- Consequences: Inappropriate angulation can cause overlapping of the SC joints, ribs, or other structures, leading to poor visualization of the joint space. This can obscure subtle abnormalities like subluxations or fractures.
3. Failure to Maintain the Correct View
- Error: Using the wrong view (e.g., standard AP view instead of the required oblique or Serendipity view).
- Consequences: The incorrect view may not reveal essential details of the joint structure, particularly if only one side of the SC joint is affected. This could lead to an incomplete evaluation of the joint, missing critical findings such as asymmetric joint space or displacement.
4. Inadequate Collimation
- Error: Over-collimation (too narrow) or under-collimation (too broad) of the X-ray beam.
- Consequences: Over-collimation may exclude parts of the SC joint, while under-collimation can capture unnecessary anatomy, reducing image contrast and adding irrelevant detail. Both errors can complicate image interpretation.
5. Poor Patient Positioning Stability
- Error: The patient moves during the exposure due to discomfort, anxiety, or lack of proper support.
- Consequences: Motion blur reduces image sharpness and can obscure critical anatomical details. This results in a loss of diagnostic clarity and often necessitates repeat imaging.
6. Incorrect Tube Angulation
- Error: Incorrect adjustment of the X-ray tube’s angle, such as using inadequate cephalad angulation for the Serendipity view.
- Consequences: Improper tube angulation can cause foreshortening or elongation of the joint structures, distorting the anatomy and making accurate assessment difficult. It may also result in overlapping bony structures, complicating the evaluation.
7. Misuse of Exposure Settings
- Error: Using incorrect kVp (kilovoltage peak) and mAs (milliampere-seconds) settings that are not optimized for the SC joint.
- Consequences: Incorrect exposure can either overexpose (too bright) or underexpose (too dark) the image, affecting contrast and the ability to distinguish subtle joint changes. This can obscure fractures, joint spaces, or soft tissue involvement.
8. Failure to Use Proper Lead Shielding
- Error: Not positioning lead aprons or other shielding correctly, which can interfere with the X-ray field.
- Consequences: Misplaced shielding may inadvertently cover parts of the SC joint, obstructing the view and rendering the image non-diagnostic, requiring a repeat X-ray.
9. Not Accounting for Patient Size and Body Habitus
- Error: Using standardized positioning without adjusting for variations in patient body size or shape.
- Consequences: Positioning that works for average-sized patients may not be suitable for those with larger or smaller body frames, leading to improper visualization of the joint. This can result in inadequate image penetration or difficulty distinguishing between joint structures.
10. Miscommunication with the Patient
- Error: Inadequate instructions to the patient regarding breath-holding or maintaining stillness during exposure.
- Consequences: If the patient breathes or moves during the X-ray, the resulting motion can blur the image, compromising diagnostic quality. Clear communication and patient preparation are crucial to minimize such errors.
11. Overlapping Structures
- Error: Inadequate separation of the SC joint from adjacent structures like ribs or the sternum.
- Consequences: Overlapping bones can obscure joint margins, hide fractures, or give the false appearance of a normal joint when abnormalities exist, impacting the accuracy of the diagnosis.
12. Lack of Appropriate Positioning Markers
- Error: Not placing side markers (left or right) or incorrect use of markers that obstruct critical anatomy.
- Consequences: Missing or misplaced markers can confuse image interpretation, especially in cases where the laterality of the SC joint pathology needs clear identification.
By understanding these common pitfalls and implementing corrective strategies, radiologic technologists can enhance image quality and diagnostic precision, ultimately improving patient care.
Conclusion
SC joint X-ray positioning is a delicate yet artful process that demands a deep understanding of anatomy, precise technical execution, and effective patient communication. By navigating the complexities of this joint with precision and care, healthcare professionals can unlock diagnostic insights critical for the effective management of SC joint conditions.